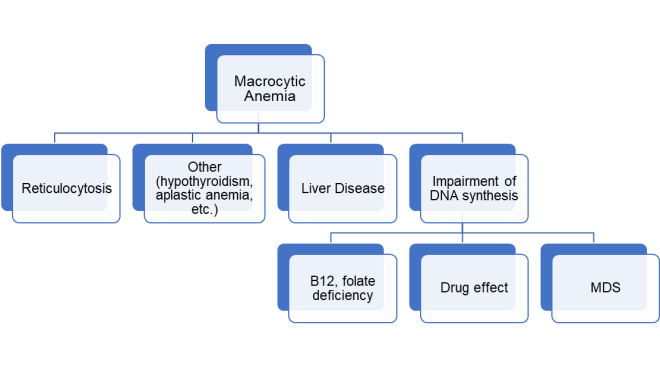
Macrocytic anemia is commonly due to folate or vitamin B12 (cobalamin) deficiency.1 Deficiency in these vitamins can be related broadly to poor intake, poor absorption, or drug interference. In patients with chronic excess alcohol consumption, both intake and/or absorption of these vitamins may be affected.
Although folate deficiency is increasingly rare in many developed countries due to mandatory folate fortification of flour and uncooked-grain, alcohol use can be associated with malnourishment severe enough to causes folate deficiency. In addition, alcohol itself can alter folate metabolism and absorption. More specifically, chronic alcohol consumption has been shown to be associated with decreased folate absorption by the small intestine, altered intrahepatic processing and distribution between the systemic and enterohepatic folate circulations as well as increased folate urinary excretion. 2 Though uncommon,3 alcohol can also be associated with a food B12 malabsorption process, whereby despite adequate intake, B12 is not released or absorbed from food. 4
But what if serum folate and B12 levels return as normal in our patient with macrocytosis? It turns out that alcohol consumption, independent of folate or B12 deficiency, may also cause macrocytosis. 5 Though the exact mechanism is unknown, it may be related to alcohol’s direct toxicity or that of its metabolites; alcohol is oxidized to acetaldehyde, which affects membranes of red blood cells (RBCs) and their precursors by forming adducts with erythroid proteins,6 and interfering with cell division.7 Interestingly, alcohol-related macrocytosis may appear before anemia is detected and can resolve within 2-4 months of abstinence.
In addition to alcohol, cirrhosis itself may be associated with macrocytic anemia caused by lipid deposition on RBC membranes.1
See also a related pearl at www.Pearls4Peers.com
References
- Hoffbrand V, Provan D. ABC of clinical haematology: macrocytic anaemias. BMJ 2011;314(7078):430–430. https://www.ncbi.nlm.nih.gov/pubmed/9040391
- Medici V, Halsted CH. Folate, alcohol, and liver disease. Mol Nutr Food Res 2013;57(4):596–606. https://www.ncbi.nlm.nih.gov/pubmed/23136133
- Bode C, Bode CJ. Effect of alcohol consumption on the gut. Best Pract Res Clin Gastroenterol [Internet] 2003;17(4):575–92. https://www.sciencedirect.com/science/article/pii/S1521691803000349
- Dali-Youcef N, Andrès E. An update on cobalamin deficiency in adults. QJM 2009;102(1):17–28. https://academic.oup.com/qjmed/article/102/1/17/1502492
- Savage DG, Ogundipe A, Allen RH, Stabler SP, Lindenbaum J. Etiology and diagnostic Evaluation of macrocytosis. Am J Med Sci [Internet] 2000;319(6):343–52. http://dx.doi.org/10.1016/S0002-9629(15)40772-4 https://www.ncbi.nlm.nih.gov/pubmed/10875288
- Latvala J, Parkkila S, Melkko J, Niemelä O. Acetaldehyde adducts in blood and bone marrow of patients with ethanol-induced erythrocyte abnormalities. Mol Med 2001;7(6):401–5. https://www.ncbi.nlm.nih.gov/pubmed/11474133
- Wickramasinghe SN, Malik F. Acetaldehyde causes a prolongation of the doubling time and an increase in the modal volume of cells in culture. Alcohol Clin Exp Res 1986;10(3):350–4. https://www.ncbi.nlm.nih.gov/pubmed/3526962
Contributed by Kim Schaefer, Harvard medical student, Boston, MA
Liked this post? Sign up under MENU and catch future pearls right into your inbox!